A great lower body strengthening exercise for both the hip and knee. If you find yourself unable to go as deep as shown in the video, only bend the knee as far as your mobility allows.
Patellofemoral Pain Syndrome (PFPS) or “Runners Knee” is one of the most common overuse injuries amongst the active population. PFPS accounts for approximately 15% of all knee pain, with females and young adults being 2 times more likely to develop symptoms due to PFPS (Boling et al, 2010).
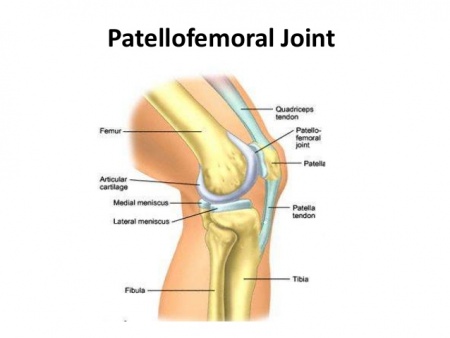
What is the Patello-Femoral Joint?
The Patello-femoral joint is one of two joints that make up the knee (see figure 1). It is comprised of the kneecap (patella) and the thigh bone (femur) and provides the attachment sites for our quadriceps and patella tendons.
How do I know if I have PFPS?
PFPS is characterised as “pain experienced around or behind the knee cap, which is aggravated by weight bearing activities that require a flexed knee such as squatting, running, jumping and hopping” (Crossley et al, 2016). It is not uncommon to also experience symptoms such as:
Creaking/grinding sensations around the knee cap
Swelling around the knee
Pain provoked by pressing the knee cap
Pain bought on by non-weight bearing activities such as sitting
Figure 1. Patello-Femoral Joint
How did I get PFPS?
Runners often develop PFPS due to a combination of several factors such as:
Muscular weakness (Quadriceps/Glutes)
Muscular tightness
Changes to training loads
Inappropriate footwear
Anatomical variations in knee cap shape/position
Changes to running style
Biomechanical abnormalities
What can I do to recover?
Currently, the best treatment supported by research is STRENGTH!!!
Strength interventions have been shown to be most effective in relieving pain and improving function in individuals with PFPS. Exercise selection should be patient specific and target the hip external rotators/hip abductors (Glut Medius) as well as the knee extensor muscles (Quadriceps) due to their roles in knee biomechanics (Martin et al, 2018).
The great news is approximately 90% of individuals suffering from PFPS will be completely symptom free within 6 weeks of starting a strength rehabilitation program guided by a physiotherapist.
What won’t work long term?
Amongst the literature there is a lack of strong evidence, supporting the long-term use of:
Although the majority of these things can help your pain in the short term, none have been shown to be superior to strength exercises of the quadriceps and gluteal musculature.
It hurts to run….what can I do?
Research on running mechanics has shown that stress on the Patello-femoral joint is greatest during mid stance and exceeds approximately 7x your body weight. This can be largely increased with
Slower speeds of running (Increase knee flexion)
Large vertical oscillation
Cross over style running
Excessive body twisting
Excessive body twisting
Ways in which you can alter your running technique to reduce knee joint stress by 15-20% are:
Maintain space between your knees when running (knee window)
Increase running cadence by 10%
Minimise excessive body twisting
How can I prevent getting sore knees?
Currently the best evidence for preventing future patella issues besides maintaining your strength is by assessing and monitoring acute: chronic training volumes in term of distance covered (Km). Acute increases in training volume should be no greater than a factor of 1.5 or you place yourself at an increased risk of suffering a subsequent injury.
We have covered this in depth in our blog titled Our Top 3 injury prevention strategies, which can be accessed by the link below:
Controversy exists regarding the optimal treatment of a torn ACL and whether surgery is necessary.
Australia has an extensive ACL problem with the highest rates of rupture in the world at 10,000 per year (Moses, Orchard, & Orchard, 2012). This is due to grass types and the popularity of cutting/change of direction sports such as netball, AFL and soccer.
Of these ruptures, Australia also has the highest rates of ACL surgery in the world at 90%, with only 10% of patients choosing conservative management. The decision to operate comes as a big one, with surgery costing between $5,000-$15,000.
How Does it Occur?
ACL injuries usually occur landing from a jump, pivoting or decelerating. The vast majority (70-80%) are non-contact injuries, usually related to biomechanical issues such as poor landing mechanics. The other 20-30% are contact injuries resulting from a direct blow or perturbation, such as a collision or being knocked mid-jump or run. For these reasons, ACL injury is common in sports such as skiing, AFL, netball, soccer, basketball and gymnastics.
Does Gender matter?
While more males suffer ACL injury on the whole, there is a gender bias towards females sustaining ACL injury. When exposed to the same level of activity (training & game time), females have a 2-8x higher risk of rupture.
Other risk factors
Extrinsic – (outside of the individual)
Dry fields, artificial turf
Game intensity – rates compared to training intensity
Grade of match – quality increases risk e.g. elite higher risk vs recreational
Greater torsional resistance – more cleats in shoes = torsion and risk
Intrinsic
Females have a higher rate of ACL injuries due to:
Hormonal effects: laxity, strength, fatigue-ability (however no conclusive evidence of menstrual cycle risk)
Decreased hamstring strength
Biomechanical – landing mechanics (females land stiffer with less hip bend)
Trunk strength / control
Some other intrinsic risk factors apply to both males and females
Greater BMI, weight, age
History of previous ACL reconstruction
Surgery vs Non-Operative Management
Several factors come into consideration when deciding between operative or conservative management. Not all ACL injuries require an ACL reconstruction. With the latest data (up to 2022), it looks like up to 50% of torn ACL’s can heal naturally and this may be aided by the use of a brace to lock the knee at 90deg for at least 4 weeks. We also know that many people can cope without an ACL at all. Each case should be assessed individually and a discussion should be had between the patient, physiotherapist and surgeon as to the best course of action required.
The following factors may help guide the decision to have surgery or not.
The following factors may contribute to a decision to AVOID surgery.
A type 1 tear where the ACL has not pulled away from the femoral attachment
A partial tear
Older age (>40)
Not participating in any sports that require repetitive pivoting
Functional knee stability – no repeat episodes of “giving way”
Success with rehabilitation. The current recommendations are for EVERY athlete who suffers an ACL injury to undergo at least 8-12 weeks of rehabilitation before considering surgery
Isolated ACL injury. E.g. no other tissues were damaged
The following factors may contribute to a decision to UNDERGO surgery.
A type 3 tear with femoral avulsion
Younger age
Participation in pivoting sports
**Knee Instability – recurrent episodes of giving way
Individuals that do rehab (exercise + strengthening) prior to surgery have superior outcomes to those that have early surgery. Delaying surgery allows for better resolution of joint trauma prior to second trauma (surgery) to the knee. It also allows time to develop better pre-op muscle strength and neuromuscular control. This enables the individual to enter surgery with a better knee outcome score, which is prognostic for better 5-year outcome.
Interestingly, a 2019 study showed that 45% of those who were originally classified as being unable to cope without an ACL became a potential coper after just 5 weeks of exercise rehab (Thoma et al., 2019).
Return to Sport Rates
Only 1/3 return to pre-injury level of sport 12 months post-op ACL repair.
90% of patients RTS after an ACL injury, only 50% return to pre-injury activity level
~30% of people never return to sport!
Re-Injury Risk
Graft re-rupture rate after 10 years is 6%
1 in 3 patients <20yrs age that return to sport will sustain a second ACL injury within the first two years after repair – the greatest risk is in 1st year post op
Athletes who return to hard cutting/pivoting sports earlier than 1 year post-op were 6x more likely to sustain a 2nd ACL injury upon return to sport irrespective of age (Grindem, Engebretsen, Axe, Snyder-Mackler, & Risberg, 2020)
Young athletes <25 years who return to high risk cutting/pivoting sports have a 30-40x greater risk of sustaining a second ACL injury.
Long-Term Outcomes
50% of people will develop arthritis 20 yrs post injury regardless of surgery or not
Arthritis risk higher after surgical repair but have better stability and less secondary meniscus tears compared with conservative
The risk of developing arthritis increases if the original injury also involved a meniscus tear
Take home messages
Many people can function normally without an ACL
Surgery can have significant financial costs ($5-$15k) and there is still a risk of re-rupture (6%)
5 weeks of exercise rehab should be performed following ACL injury, prior to considering to identify potential “copers”
Knee function is the same at 2-yrs and 5-yrs post injury, regardless of surgery or not
Surgery may still be the course of best action for high-level, younger athletes who wish to return to cutting/pivoting sports OR those with instability/giving way who have failed at least 5 weeks of rehabilitation.
References
Filbay, S. R., Ackerman, I. N., Russell, T. G., & Crossley, K. M. (2017). Return to sport matters-longer-term quality of life after ACL reconstruction in people with knee difficulties. Scand J Med Sci Sports, 27(5), 514-524. doi:10.1111/sms.12698
Grindem, H., Engebretsen, L., Axe, M., Snyder-Mackler, L., & Risberg, M. A. (2020). Activity and functional readiness, not age, are the critical factors for second anterior cruciate ligament injury – the Delaware-Oslo ACL cohort study. Br J Sports Med. doi:10.1136/bjsports-2019-100623
Moses, B., Orchard, J., & Orchard, J. (2012). Systematic review: Annual incidence of ACL injury and surgery in various populations. Res Sports Med, 20(3-4), 157-179. doi:10.1080/15438627.2012.680633
Thoma, L., Grindem, H., Logerstedt, D., Axe, M., Engebretsen, L., Risberg, M. A., & Snyder-Mackler, L. (2019). Coper Classification Early After ACL Rupture Changes With Progressive Neuromuscular and Strength Training and Is Associated With 2-Year Success: Response. Am J Sports Med, 47(11), NP65-NP66. doi:10.1177/0363546519863309
The single leg squat is a basic but fantastic measure of overall function of the lower limb. It tests both strength and flexibility of the ankle, knee and hip. Having a good single leg squat can dramatically reduce your risk of sustaining a lower limb injury.
The 3 main points we look for are:
Does the knee track straight forward over the toes (good) or does it collapse inwards (poor)?
Does the trunk stay centred over the foot (good) or does it sway out to the side (poor)?
Is there an even contribution from ankle, knee and hip (good) or is there a preference/dominance of one of the joints (poor)?
These exercises are designed to reduce the risk of suffering common footballing injuries.
The most common injuries, ranked in order are:
Hamstring Tear
Knee Ligament/Meniscus Injury
Ankle Ligament Injury
Groin Strain/Pain
To address the strength and control deficits that can increase the risk of these injuries, the following exercises should be completed at least twice a weak, at the END of a training session OR by themselves in a separate session.
Nordic Hamstring Curl. Perform as slowly as possible. Do 3 sets of 8 reps.
Copenhagen Adductor Exercise. Do 3 sets of 12 each leg.
Lateral ankle/knee stability jumps. Do 3 sets of 8.
Single leg Agility jumps over line. Do 3 sets of 20 each leg.