 Causing Your Headache")
Does your jaw click? Do you grind your teeth or wake up in the morning with sore teeth? Does it hurt to open your mouth all the way? Or hurt to chew? These are all signs that there may be an issue with your temporomandibular joint (TMJ).
Simple Anatomy
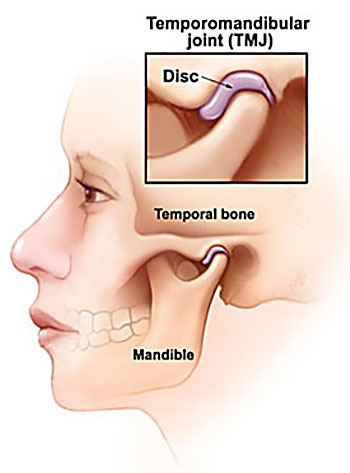
The TMJ is a common, yet poorly understand cause of headache and neck pain. It is actually a fairly simple structure and acts like many other joints in the body with surrounding muscles acting on the joint to produce movement up and down and side to side. It has a small disc inside the joint that allows for smooth movement of the joint. It is this disc translating forwards/backwards that can cause “clicking” when you open and close.
Cause of pain in the TMJ
There are 2 main structures which are sources of pain in the TMJ.
1) The muscles – in particular the large masseter muscle that sits on the outside of the jaw. If you place a finger on the outside of your jaw and clench, you can feel this muscle bulge into your finger. The other muscles are the medial and lateral pterygoid muscles which sit inside the mouth and help to open and close and move the jaw forwards. These muscles can either get tight/overworked (particularly if your stressed) or can also become weak.
A recently published study by Greenbaum et al (2021) found that the muscles of the TMJ are the primary cause of headache from TMJ disorders and 38% patients with muscular TMJ disorders will develop headache.
2) The Joint, including the small disc that sits inside the joint. The joint has 2 main movements. 1 is to “roll” open and closed and the other is movement side to side. The disc helps to cushion the joint when we clench and also aids the lubrication of the joint.
The joint can become painful either due to trauma, developing poor chewing mechanics or, again, if there is some underlying stress/anxiety causing jaw clenching at night. Greenbaum’s conclusions also found that if the primary cause of jaw pain is from the joint, there is almost a 0% chance that you will develop a headache.
How can the TMJ cause a headache?
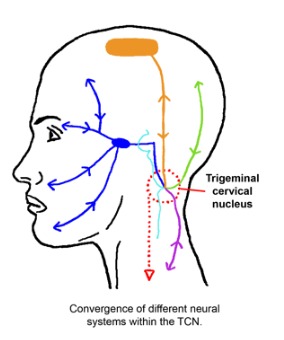
As stated above, the muscles of the TMJ are the primary cause of headache. These muscles can refer into the head due to a phenomena known as “convergence”. This is where the nerves that supply the jaw muscle (in blue in the pic below) converge/communicate via the same nerves that supply the head (in green and orange).
All these nerves share a common central nucleus, almost like a roundabout, where these nerves all meet then go there separate ways again. Our brains can get a little confused as to the source, so we end up experiencing pain in both the jaw and the head.
Treatment
Treatment really depends on what we find during the assessment. For example, in order to assess for muscle weakness or overactivity of the pterygoids we conduct some specific movement and strength tests. If we do find an issue with overactivity, then we may do a muscle release on the pterygoids then reassess your jaw movement again.
The can also be a link between poor posture and TMJ pain. This test to determine if there is a link is quite simple. We place the patient in a “poor posture” position i.e. slumped with head forward and ask them to open and close. We then place the patient in an upright position, with head back and ask them to open and close again. If posture is contributing to the symptoms, the patient will report less pain and also be able to open their jaw further.
If you do have jaw pain, or potentially a headache that you now think might be originating from your jaw, please don’t hesitate to get in touch with us at clinicalphysiostives.com.au
Does your jaw click? Do you grind your teeth or wake up in the morning with sore teeth? Does it hurt to open your mouth all the way? Or hurt to chew? These are all signs that there may be an issue with your temporomandibular joint (TMJ).
Simple Anatomy
The TMJ is a common, yet poorly understand cause of headache and neck pain. It is actually a fairly simple structure and acts like many other joints in the body with surrounding muscles acting on the joint to produce movement up and down and side to side. It has a small disc inside the joint that allows for smooth movement of the joint. It is this disc translating forwards/backwards that can cause “clicking” when you open and close.
Cause of pain in the TMJ
There are 2 main structures which are sources of pain in the TMJ.
1) The muscles – in particular the large masseter muscle that sits on the outside of the jaw. If you place a finger on the outside of your jaw and clench, you can feel this muscle bulge into your finger. The other muscles are the medial and lateral pterygoid muscles which sit inside the mouth and help to open and close and move the jaw forwards. These muscles can either get tight/overworked (particularly if your stressed) or can also become weak.
A recently published study by Greenbaum et al (2021) found that the muscles of the TMJ are the primary cause of headache from TMJ disorders and 38% patients with muscular TMJ disorders will develop headache.
2) The Joint, including the small disc that sits inside the joint. The joint has 2 main movements. 1 is to “roll” open and closed and the other is movement side to side. The disc helps to cushion the joint when we clench and also aids the lubrication of the joint.
The joint can become painful either due to trauma, developing poor chewing mechanics or, again, if there is some underlying stress/anxiety causing jaw clenching at night. Greenbaum’s conclusions also found that if the primary cause of jaw pain is from the joint, there is almost a 0% chance that you will develop a headache.
How can the TMJ cause a headache?
As stated above, the muscles of the TMJ are the primary cause of headache. These muscles can refer into the head due to a phenomena known as “convergence”. This is where the nerves that supply the jaw muscle (in blue in the pic below) converge/communicate via the same nerves that supply the head (in green and orange).
All these nerves share a common central nucleus, almost like a roundabout, where these nerves all meet then go there separate ways again. Our brains can get a little confused as to the source, so we end up experiencing pain in both the jaw and the head.
Treatment
Treatment really depends on what we find during the assessment. For example, in order to assess for muscle weakness or overactivity of the pterygoids we conduct some specific movement and strength tests. If we do find an issue with overactivity, then we may do a muscle release on the pterygoids then reassess your jaw movement again.
The can also be a link between poor posture and TMJ pain. This test to determine if there is a link is quite simple. We place the patient in a “poor posture” position i.e. slumped with head forward and ask them to open and close. We then place the patient in an upright position, with head back and ask them to open and close again. If posture is contributing to the symptoms, the patient will report less pain and also be able to open their jaw further.
If you do have jaw pain, or potentially a headache that you now think might be originating from your jaw, please don’t hesitate to get in touch with us at clinicalphysiostives.com.au
