We show you the best 3 hamstring exercises to improve strength, speed and prevent injury.
In our latest video, Jin Su Jung, one of Australia’s top sprinters with a PB of 10.27, demonstrates our top 3 hamstring exercises to develop strength, speed and most importantly, prevent injury.
The most important thing to remember when prescribing hamstring exercises is that the exercise should mimic, as closely as possible, the actions, loads and positions that hamstrings go through, particularly at the point in the gait cycle that they tend to tear. This point is when the hamstring quickly moves from an eccentric (lengthening phase) to a concentric (shortening phase) which happens when the hip is flexed out in front and the knee moves from extension (straightening) to flexion (bending). If the hamstring is not strong enough to make the transition quickly, it will fail and “tear”.
The exercises
Do 3- 4 sets of 6-8 reps of each, twice a week. Try to NOT do it 24 hours PRIOR to a high intensity running/sprint session. Try to make the transitions from lengthening to shortening as quickly as possible and in a PAIN FREE manner.
Exercise no.1 – Nordic hamstring curl
Not my favourite as it is a double leg exercise and hamstring injuries are a single leg injury, however, it is the only single exercise thus far that has been proven, in 2 different studies, to reduce hamstring injury rates (Van der Horst et al 2015 & Peterson et al 2011).
Tips: Don’t “drop” at the end of the movement. If you are not strong enough to go all the way down then stop when you feel you are about to fail and pull back. Try to go a little lower each week.
Exercise no.2 – Single leg glute/ham raise on GHD machine
Tip: Keep the knee flexed (don’t let it straighten) the entire time and try to produce the movement through your hip/glute. MUST BE DONE AS A SINGLE LEG EXERCISE.
Exercise no.3 – Single leg skateboard hamstring curl/glute raise
Tip: Again do not let the knee straighten all the way. Skateboards are available at Kmart for about $30. Well worth it!
If you have had a hamstring tear then approach these exercises slowly. There are many other factors that can contribute to hamstring tears so if you do get recurrent hamstring tears or pain then please book yourself in to see an experienced musculoskeletal physiotherapist.
The important stuff you need to know about rotator cuff injuries.
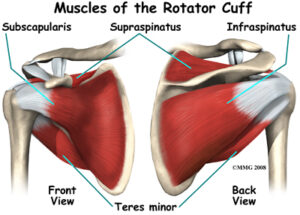
The rotator cuff is a very important group of four small muscles (supraspinatus, infraspinatus, subscapularis & teres minor) that connect the upper arm to the shoulder blade (see image). Their main role is to not only move and control movements of your shoulder but to also provide dynamic stability to the shoulder joint.
Unfortunately, rotator cuff tears, which can occur to any one of these muscles, are one of the most common causes of shoulder pain and disability in both the sporting and general populations and can make everyday tasks increasingly difficult and often very painful.
Research has shown that the risk of developing a rotator cuff tear increases with age. Jobs and sports that require repetitive overhead work also increase the risk of rotator cuff injury. Jobs such as construction, carpentry, electricians and painters as well as sports that require overhead movements such as swimming, baseball, cricket and volleyball can all predispose the shoulder to injury.
How do rotator cuff tears occur?
Rotator cuff tears generally develop as a result of either:
Traumatic events – Such as a fall onto an outstretched arm or lifting a heavy object
Non- traumatic events – Such as excessive repetitive use or normal age related wear and tear
How do I know if I have a rotator cuff tear?
Symptoms of a rotator cuff tear can vary from person to person, however, common findings include:
Pain on the side or back of the shoulder
Pain in the upper arm.
Reduced shoulder movement and pain associated with overhead tasks such as changing a lightbulb or reaching for the top shelf of a kitchen cabinet or other tasks such as reaching behind your back or out to the side.
A feeling of weakness with shoulder movements
Pain sleeping on the affected side
Should I get a scan?
Imaging studies, both Ultrasound and MRI, have shown that the prevalence of rotator cuff tears in asymptomatic (symptom free) individuals is approximately 50% in those aged between 40 to 60 years of age, and as high as 80% in those older than 80 years of age. (Harris et al, 2012). This means that if a tear is present on an ultrasound or MRI it may just be due to the natural ageing process and not related to your shoulder symptoms at all.
If you have shoulder pain and are unsure whether you require imaging, your physiotherapist will be able to determine if your pain is caused by the presence of a tear or any other underlying factors.
How can physiotherapy help?
Research has shown that physiotherapy management, specifically strength training, should by the first treatment option for rotator cuff injuries (Ladermann et al, 2015; Ainsworth et al, 2007; Collin et al, 2015).
Rotator cuff tears account for over 50% of all shoulder conditions seen by physiotherapists on a regular basis (Donatelli, 2011).
The first thing that we will determine is whether your symptoms are in fact due to a tear to the rotator cuff. This is achieved by a thorough assessment of your shoulder, neck and upper back including:
A detailed history of your injury
Clinical examination of your shoulder movements and strength
Special orthopaedic shoulder tests
Examination of your neck and upper back movements
Palpation of your shoulder muscles and surrounding structures
Determine if imaging is required
Determine if you need to see an orthopaedic specialist
Set specific, individualised rehabilitation goal
What does treatment entail?
A 1 hour initial consultation is recommended for your first session. After your assessment, treatment may include:
Treatment and advice for pain reduction
Hands-on manual therapy for restoration of normal shoulder movement
Restoration of normal neck and upper back movement
Lower back pain is the single most common musculoskeletal complaint in the world. Up to 85% of the population will complain of low back pain at some stage in their lives. It is also the 3rd most common reason people will visit a GP.
Lower back pain can be broken into 2 broad types.
Central Low Back Pain – pain that does not dominate one side and is experienced generally across the entire lower back region.
Unilateral Low Back Pain – pain that is experienced on one side only.
It is this second that we are going to talk about.
Whilst there are other possible causes of unilateral low back pain, the most common cause we see is actually the hip. The reason is that when we load the lower limbs in tasks such as getting out of a chair, walking, running, climbing stairs, this load is transferred from the ankle, through the knee, then to the hip and then finally the lower back. If the hip is not functioning optimally, this load will bypass the hip and be transferred straight into the lower back on the same side.
Because the hip has significant movement in all 3 planes (forwards, backwards, side to side and rotation) it plays a much more complex role than the ankle and knee which move predominantly in 2 and 1 planes respectively. Back pain on one side can also be attributed to the ankle or knee but these are less common causes.
What does the evidence say?
Sadeghisani and colleagues in 2015 conducted a review of all the published literature of hip range of motion and its relationship to low back pain. They concluded that hip range of motion testing, particularly hip internal rotation, should be a standard, routine part of an examination for patients with low back pain.
Eyvazov and colleagues in 2016 conducted a study on 28 patients booked in for a hip replacement found that their concomitant lower back pain was reduced by 50% after their surgery.
A study earlier this year by Prather and colleagues on 101 patients with low back pain found that those with positive hip examination findings (predominantly reduced hip flexion and internal rotation range of motion), had more pain and poorer function compared to those with normal hip findings.
Sorenson and collegues (2016) found that asymetrical performance of hip abduction (moving the leg out to the side) was a significant risk factor for people that get low back pain when standing.
How do we find out if your hip is the problem?
There are 2 parts to the assessment.
Assessment of your lumbar movements in positions that you have reported to be a problem. For example if you get your pain during or after running, then we’ll get you on the treadmill to have a look at what happens around the hip when you run. If you get the pain simply getting out of a chair, then we’ll examine that movement. We will often find that due to reduced hip function, there are abnormal compensatory movements that occur in the lumber spine.
Assessment of hip strength and range of motion on the same side. Often if the pain is related to the hip, there will be deficits in either strength or range of motion or both, on the same side as your pain. Studies show that the 2 most important movements to assess are hip flexion and hip internal rotation.
If you are suffering from lower back pain one one side then don’t be afraid to get in touch with us to have your hip checked out.
Ellison JB, Rose SJ, Sahrmann SA. Patterns of hip rotation range of motion: a comparison between healthy subjects and patients with low back pain. Phys Ther. 1990; 70(9): 537-541.
Chesworth BM, Padfield BJ, Helewa A, et al. A comparison of hip mobility in patients with low back pain and matched healthy subjects. Physiotherapy Canada. 1994; 46: 267-74.
Eyvazov K, Eyvazov B, Basar S, Nasto LA, Kanatli U. Effects of total hip arthroplasty on spinal sagittal alignment and static balance: a prospective study on 28 patients.Spine J. 2016 Nov;25(11):3615-3621. Epub 2016 Jul 15.
Prather H, Cheng A, Steger-May K, Maheshwari V, Van Dillen L. Hip and Lumbar Spine Physical Examination Findings in People Presenting With Low Back Pain, With or Without Lower Extremity Pain.Orthop Sports Phys Ther. 2017 Mar;47(3):163-172. doi: 10.2519/jospt.2017.6567. Epub 2017 Feb 3.
Sorensen CJ, Johnson MB, Norton BJ, Callaghan JP, Van Dillen LR. Asymmetry of lumbopelvic movement patterns during active hip abduction is a risk factor for low back pain development during standing.Mov Sci. 2016 Dec;50:38-46. doi: 10.1016/j.humov.2016.10.003. Epub 2016 Oct 13.
Sadeghisani M, Manshadi FD, Kalantari KK, Rahimi A, Namnik N, Karimi MT, Oskouei AE. Correlation between Hip Rotation Range-of-Motion Impairment and Low Back Pain. A Literature Review.Traumatol Rehabil. 2015 Oct;17(5):455-62. doi: 10.5604/15093492.1186813.
Sitting or standing, push toes down into the floor so your arch raises slightly. Keep you heel on the ground. Hold for 10 seconds and repeat x 5 each foot.
Calf raises with band around ankles. Raise up onto your toes whilst pulling outwards into band. Do 3 sets of 20. To progress, try doing it on one leg at a time and/or make the band tighter.
These 2 exercises are designed for people with quite severe lateral elbow pain that have difficulty gripping/lifting even light objects.
1) Isometric Wrist Extension with 1kg dumbbell.
Start with 3x10sec holds. If pain-free, progress to 3x30sec holds or increase the weight. If you can tolerate doing this every day for 1 week, progress to exercise no.2
2) Eccentric Wrist Extension
Do 3 sets of 15 reps with 1kg. If pain-free, add an extra 1kg. Complete this exercise every second day.